The surgeons at OIP are partners in your mobility, using knowledge to help you recover faster. Experience world-class surgical expertise here in Central PA. Schedule a consultation with our team today to see if an anterior hip replacement is right for you.
Anterior Hip Replacement
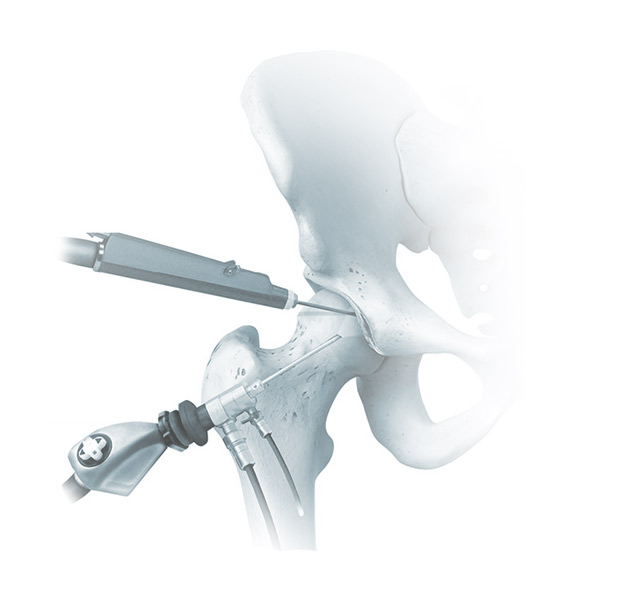
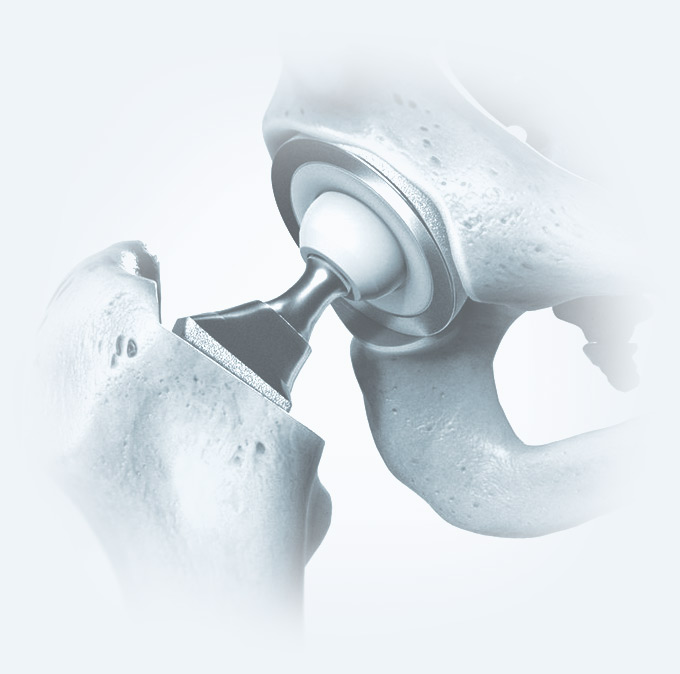
An anterior hip replacement is a minimally invasive surgical technique that accesses the hip joint from the front of the leg rather than the side or back. This approach allows a surgeon to work between the muscles rather than cutting through them to reach the joint, as previously done in traditional posterior hip replacement surgery. As a result, surgeons can replace the damaged joint with less trauma to the surrounding soft tissues, encouraging faster healing.
At the Orthopedic Institute of PA (OIP), our team of experts can help relieve your hip joint pain, increase your mobility and improve your quality of life.
4.9 stars 4.95 out of 5 (1611 reviews) About star rating